Depression is a common and treatable condition
Good health is not limited to physical health.1 Mental health and well-being are also important. Therefore, screening and treatment for depression is an important priority for the Living Well goal. Depression is a common and treatable condition which can have serious health consequences if left untreated.2 Let’s Get Healthy California seeks to reduce the number of adults and adolescents (teens) who experience a major depressive episode. Additional data needs to be developed in order to provide a measure for effectively diagnosing and treating depression in adolescents and adults.3
For resources regarding Mental Health services for various populations, please see the Mental Health Services Division website.
For details on County Mental Health Plans, including links on depression screening resources, please see the Mental Health Quality Improvement Work Plan website.
Adult Depression
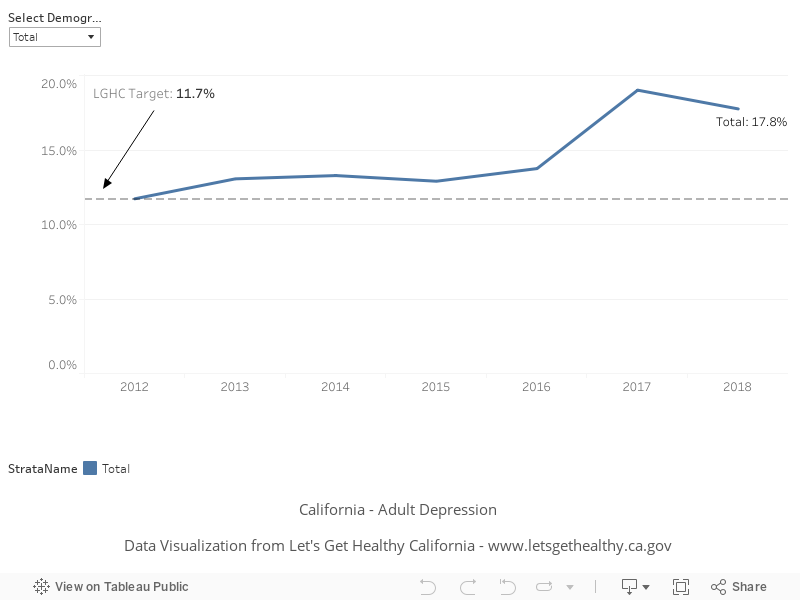
In 2012 (baseline year), 11.7% of adults were told they had a depressive disorder. The most recent data available show 17.8% (2018). We hope to reach a target of no increase in prevalence compared to baseline by 2022.
Baseline
11.7%
Target
See text
Indicator Highlights

California Reducing Disparities Project
California Reducing Disparities Project is a statewide policy initiative to develop strategies to transform the public mental health system and identify solutions for historically unserved, underserved, and inappropriately served communities.
The effort focuses on identifying, and evaluating community-based promising practices in each of five targeted populations: African Americans, Asians and Pacific Islanders (API), Latinos, Lesbian, Gay, Bisexual, Transgender, Queer, and Questioning (LGBTQ), and Native Americans.
There has not been a project of this scope before; one that recognizes and elevates community practices and identifies strategies for systems change. Throughout this process, California will present this work on the national stage so that other states can learn from our efforts.
Culturally Competent Care
In California, almost one in six adults has a mental health need, including people of all races and ethnicities and all social, and economic, and education levels, but there are striking disparities in access to treatment and services.1 Issues such as stress and trauma related to immigration, racial discrimination, poverty, language barriers, and cultural differences play an especially important role, not only in the risk of having mental illness, but also in access to quality mental health services.4
Depression is a risk factor for the development of cardiovascular conditions and other chronic disease.4
Data Snapshot: Trends and Disparities
Almost three of four Mexican Americans who have a diagnosable mental disorder and need services remain untreated.4
More Native Americans and African Americans under 35 have seriously thought about committing suicide (27% and 18% respectively), compared to other racial/ethnic groups.4
White men have the highest age-adjusted rates of suicide (22 per 100,000 population) among all racial/ethnic groups.4
Proportion of Adults Who Were Told They Had a Depressive Disorder, Over Time
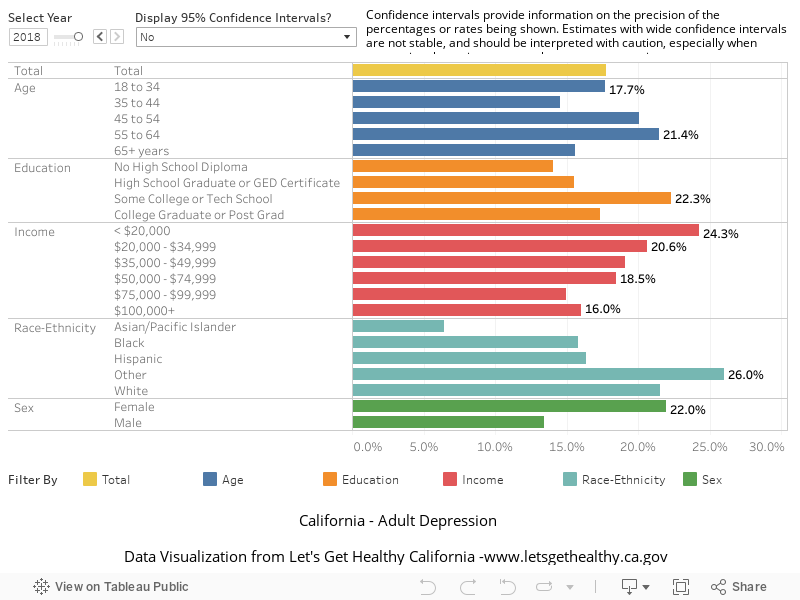
Proportion of Adults Who Were Told They Had a Depressive Disorder, by Demographic Category
|
Stories & Solutions

California Reducing Disparities Project – Phase 1
Focuses on developing strategies to transform the public mental health system and identifying community-based promising practices in each of the five targeted populations. Read more »
California Reducing Disparities Project – Phase 2
Focus on funding and evaluating the promising practices identified in Phase 1, as well as advancing the strategies outlined in this plan. There has not been a project of this scope before; one that recognizes and elevates community practices and identifies strategies for systems change. Throughout this process, California will [...]
California Reducing Disparities Project – Stakeholder Generated Reports
Stakeholder workgroups focusing on five populations developed individual Population Reports that included recommendations for reducing disparities and removing barriers to accessing programs and services, along with an inventory of community-defined evidence and promising practices that could support efforts to reduce disparities.
Share Your Story
Want to engage in moving the dial on the Living Well goal? Share your impact story!


