70 percent of Californians want to be at home at end of life1
A large majority of Californians say they would prefer a natural death if they became severely ill, rather than receiving treatments that artificially lengthen their life span. Although most individuals say that they would prefer to die at home, many die in hospitals where they often receive highly aggressive care.1
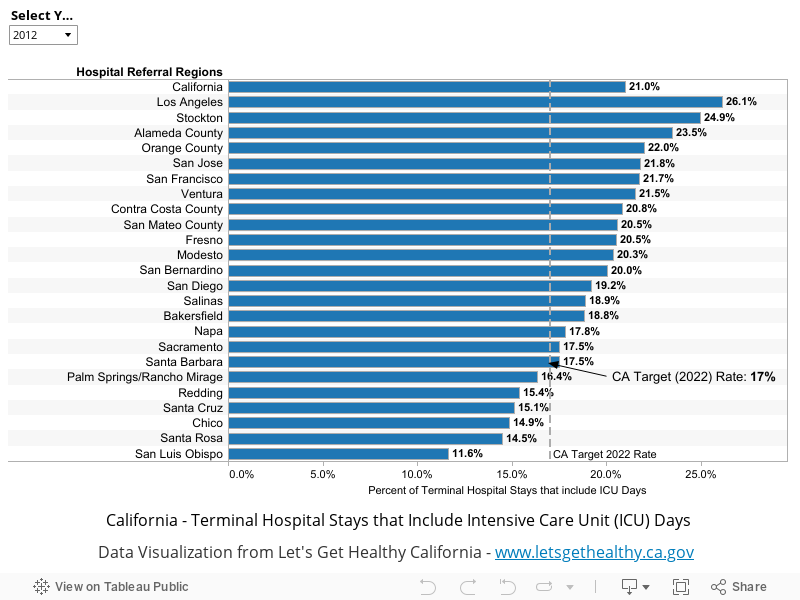
Use of an ICU within a hospital stay at the end of life is one indicator of a potential mismatch between patient preferences and care delivered.1 Tracking the number of hospitalizations that end in death and included an ICU stay is one way of measuring our ability to provide care to patient preferences.
Indicator Progress
In 2010 (baseline year), 22.0% of terminal hospital stays included ICU stays. The current value in 2012 was 21.0%. The updated 2034 target is to be determined (TBD).
More Data about Terminal Hospital Stays that Include Intensive Care Unit (ICU) Days
Baseline
22.0%
Target
TBD
Indicator Highlights
How to Make Advance Care Planning Easier
How to Make Advance Care Planning Easier connects with older adults to provide education to them about advanced care directives. The development and implementation of the PREPARE website (www.prepareforyourcare.org) guides patients through an easy-to-understand format that helps them take the necessary steps to communicate their wishes to loved ones and medical care providers. Read more »
Percent of Terminal Hospital Stays that Included an ICU Admission
|
Stories & Solutions

Innovation Conference: End of Life Breakout Session
Moderated panel discussion among Innovation Challenge finalists on interventions to address End of Life.
Medical-Legal Partnership for Seniors
The Medical-Legal Partnership for Seniors provides legal assistance to lower income adults assisting them with health and financial advice, as well as advance care planning.
Aging With Dignity at Home
Aging with Dignity at Home, AltaMed’s Program of All-Inclusive Care for the Elderly (PACE) allows seniors to receive coordinated medical, social, dental, nutritional and rehabilitative services, including Adult Day Health Care (ADHC) close to their homes and within the community.
UCLA Health/Coalition for Compassionate Care of California Advance Care Planning Initiative (ACPI)
The Coalition for Compassionate Care of California (CCCC) is partnering with the UCLA Health System to develop and test an innovative comprehensive advance care planning model that routinely receives patient preferences through a standardized process that ensures that these preferences are recorded and that they can be retrieved and honored at critical times.

Death Over Dinner
Parties where participants have dinner together and created a safe place to have the conversation about the end of life.

Being Mortal
Frontline explores the intersection of life, death, medicine, and what matters in the end.


Palliative Pooches: When Dogs Make the Rounds
Learn about the service that therapy dogs provide by supporting and comforting patients and doctors in palliative care settings.
Dying in California: A Status Report on End-of-Life Care
Dying in California serves as a snapshot of the state's progress in end-of-life care, as measured against the recommendations made in the Institute of Medicine's influential 2014 report Dying in America: Improving Quality and Honoring Individual Preferences Near the End of Life.
Share Your Story
Want to engage in moving the dial on the End of Life goal? Share your impact story!


