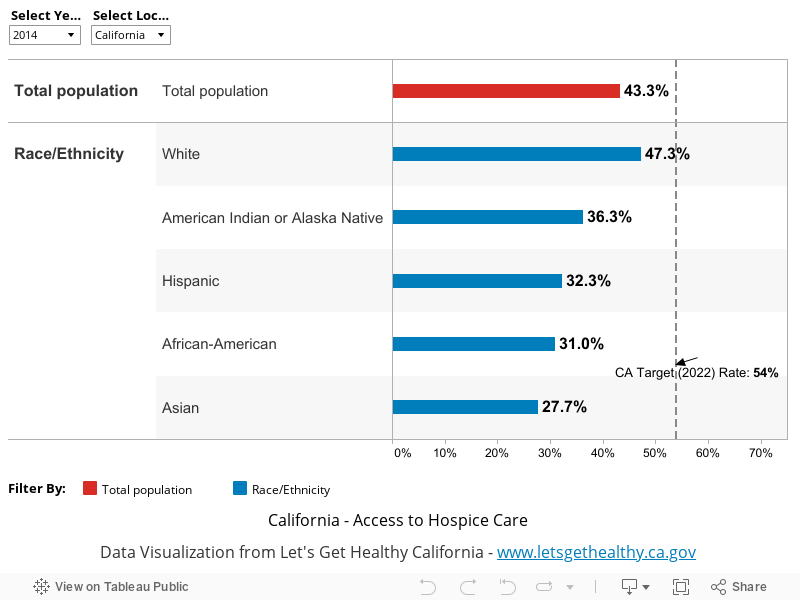
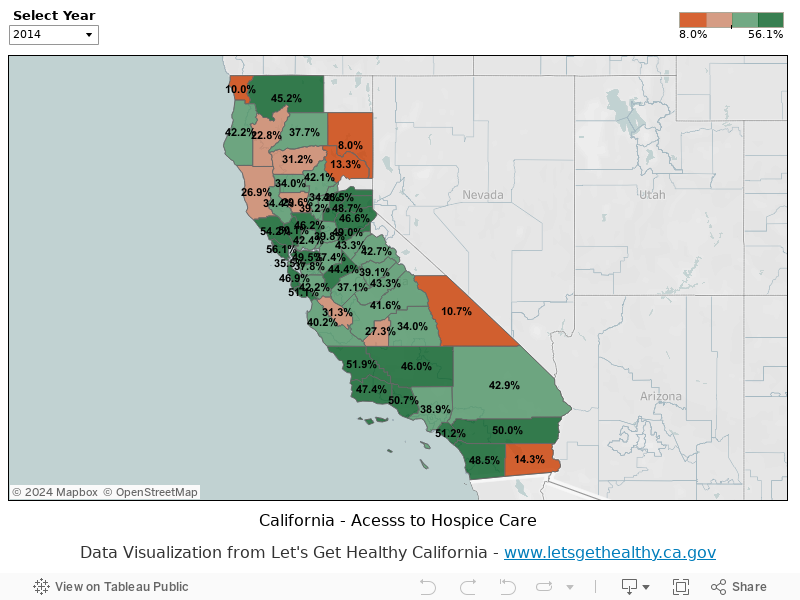
Indicator: Hospice enrollment rate
Description: Hospice is a type of palliative care that is typically available to individuals with a life expectancy of six months or less. The objective of hospice is not to cure illness, but instead to minimize the physical, emotional, and spiritual suffering that is often experi-enced by patients towards the end of life. The patient-centered approach that is at the heart of the hospice model, coupled with clinical expertise in pain and symptom management, often lead to superior outcomes for patients and families who receive hospice care, as compared to those who receive usual care. Unfortunately, not all patients or health care providers understand the benefits that hospice can offer. Too often, patients and families are not given the information they need to determine if hospice is right for them. As a result, many patients and families who might benefit from hospice do not utilize this important and proven resource. Tracking the proportion of individuals who die who utilize hospice is one way of assessing our state’s ability to provide the best care possible to individuals with terminal illnesses.
Data Limitations: Outcomes are derived from Medicare Fee-for-service (FFS) claims data for patients age 66-99 years, with one or more of nine chronic illnesses: cancer or leukemia, congestive heart failure, chronic pulmonary disease, dementia, diabetes with end organ damage, peripheral vascular disease, chronic renal failure, severe chronic liver disease, and coronary artery disease. Use patterns in this population may differ from those seen in groups with other types of illnesses or insurance coverage, such as Medicare Advantage (HMO) or Medi-Cal.
Further, tracking hospice length of service is an important companion measure to enrollment rate. According to the National Hospice and Palliative Care Organization, in 2013 34.5% of individuals who used hospice had a length of service of 7 or fewer days. Very short length of service may be indicate that a patient and family could not yield the full benefit of hospice, and that the patient have been subjected to a burdensome transition in the final days of life. One national study found that in 2009, 28.4% of hospice use at the time of death was for 3 days or less; 40.3% of these very late hospice referrals were preceded by a hospitalization that featured an ICU stay.
Indicator Source: Dartmouth Atlas of Healthcare analysis of Medicare FFS claims data among patients with 9 chronic conditions: cancer or leukemia, congestive heart failure, chronic pulmonary disease, dementia, diabetes with end organ damage, peripheral vascular disease, chronic renal failure, severe chronic liver disease, and coronary artery disease.
Indicator Calculation Methodology: Denominator definition: The study population includes beneficiaries with one of nine chronic conditions who were enrolled in traditional (fee-for-service) Medicare and died during the measurement period. To allow for two years of follow-back for all patients, the population is restricted to those whose age on the date of death was 67 to 99 years, and to those having full Part A and Part B entitlement throughout the last two years of life. Persons enrolled in managed care organizations were excluded from the analysis. Numerator definition: Number of beneficiaries with one or more claims in the Hospice file. Adjustments: Rates are adjusted for age, sex, race, primary chronic condition, and the presence of more than one chronic condition using ordinary least squares regression. Research Methods description available at: https://www.dartmouthatlas.org/downloads/methods/research_methods.pdf
Data Collection Methodology: https://www.dartmouthatlas.org/downloads/methods/research_methods.pdf
Program URL Link: https://www.dartmouthatlas.org/
Geographic Granularity: State. Data are also available by Hospital Referral Regions (HRR) and Hospital Service Areas (HSA) Hospital referral regions (HRR) represent regional health care markets for tertiary medical care that generally requires the services of a major referral center. The regions were defined by determining where patients were referred for major cardiovascular surgical procedures and for neurosurgery. Each HSA was examined to determine where most of its residents went for these services. The result was the aggre-gation of the 3,436 HSAs into 306 HRRs. Each HRR has at least one city where both major cardiovascular surgical procedures and neurosurgery are performed.
HSAs are local health care markets for hospital care. An HSA is a collection of ZIP codes whose residents receive most of their hospitalizations from the hospitals in that area. HSAs were defined by assigning ZIP codes to the hospital area where the greatest proportion of their Medicare residents were hospitalized. Minor adjustments were made to ensure geographic contiguity. This process resulted in 3,436 HSAs. When these regions were created in the early 1990s, most HSAs contained only one hospital. In the intervening years, hospital closures have left some HSAs with no hospital; these HSAs have been maintained as distinct areas in order to preserve the continuity of the database.
Data categorized by:
Health payer: Outcomes reported for individuals with Medicare FFS coverage.
Age category: Outcomes are reported for individuals age 66-99
Reporting Cycle: Annually
Reporting Lag: 3 Years
Indicator Source Changes: These data were originally obtained from the California Hospice and Palliative Care Association (CHAP-CA), which conducted an analysis of Medicare claims data
National Benchmark Indicator: Same as above, national rate
National Data Limitations: California is a populous and diverse state: The health care system and payer mix are different from what exists in many other states.
Tags (Keywords): Hospice, end of life care, EOL