Adverse childhood experiences have a lasting, harmful effect on health and wellbeing.1
Adverse Childhood Experiences (ACEs) affect nearly two million children in California across socioeconomic lines, putting them at risk for health, behavioral, and learning problems.2 ACEs are traumatic childhood experiences – which include abuse, neglect, and being exposed to violence, mental illness, divorce, substance abuse, or criminal activity in the home – that often leave people more vulnerable to environments and behaviors that can lead to poor health. The more ACEs an individual has experienced, the higher their risk climbs.3
The National Survey of Children’s Health (NSCH) tracks the percent of California children who have experienced ACEs. It uses a set of questions on family, economic, and community adversity to ask parents about current adverse experiences to which their children have been exposed. This population-based survey measures adversity among California children by asking parents about the trauma their children have experienced while they are still children, compared to methods that ask adults to recall their childhood experiences, such as adult retrospective data from the California Behavioral Risk Factor Surveillance System (BRFSS).2,4
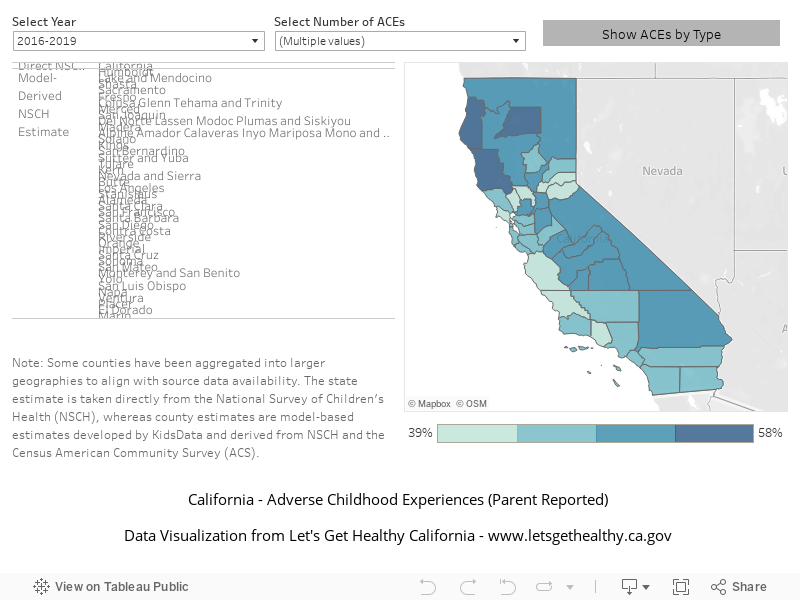
Adverse Childhood Experiences – Parent Reported
In 2016-2019 (baseline year), 36.0% of children are exposed to one or more adverse experience (parent reported). The current value from 2016-2019 was 36.0%. The updated 2034 target is to be determined (TBD).
More Data about Adverse Childhood Experiences – Parent Reported
Baseline
36.0%
Target
TBD
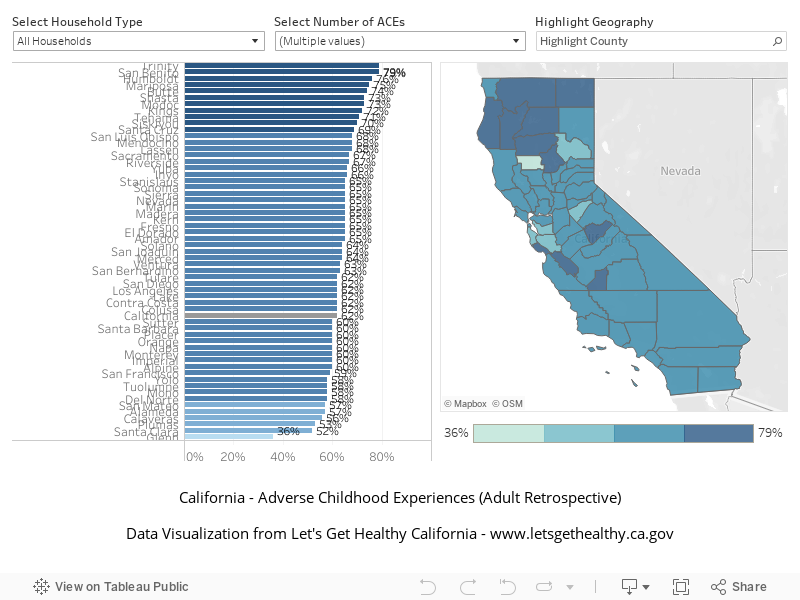
Adverse Childhood Experiences – Adult Retrospective
In 2008-2009 (baseline year), 59.0% of adults reported having been exposed to one or more adverse childhood experience before the age of 18. The current aggregated value in 2011, 2013, 2015, and 2017 was 62.0%. This indicator serves to inform and consequently does not have a target.
More Data about Adverse Childhood Experiences – Adult Retrospective
Baseline
59.0%
Target
-
Indicator Highlights
California Essentials for Childhood Initiative
The California Essentials for Childhood (EfC) Initiative seeks to address child maltreatment as a public health issue; aims to raise awareness and commitment to promoting safe, stable, nurturing relationships, and environments (SSNR&E); creates the context for healthy children and families through social norms change, programs, and policies; and utilizes data to inform actions. Utilizing a collective impact model, the EfC Initiative advances the common agenda of multiple agencies and stakeholders through alignment of activities, programs, policies, and funding so that all California children, youth, and their families achieve SSNR&E. Learn more »
ACEs Lead to Increased Risk of Negative Physical Health Outcomes
A person with four or more ACEs is:
- 2.1 times as likely to die from heart disease3,4
- 2.3 times as likely to die from cancer3,4
- 5.9 times as likely to contract a sexually transmitted infection3,4
ACEs Lead to Increased Risk of Negative Mental Health Outcomes
A person with four or more ACEs is:
- 4.4 times as likely to suffer from depression 3,4
- 4.7 times as likely to seek help from a mental health professional 3,4
- 30.1 times as likely to attempt suicide 3,4
ACEs Lead to Increased Risk of Substance Use
A person with four or more ACEs is:
- 2.9 times as likely to smoke 4
- 7.4 times as likely to experience alcoholism 4
- 10.3 times as likely touse injection drugs 4
Early Intervention is Key
Screening for ACEs in children as early as possible and providing children and their families with the support services they need is a critical step to prevent and undo the existing and future harm to children’s brains and bodies caused by toxic stress. 5
- Working to educate parents and caregivers about the impact a child’s environment and
exposures may be having on children’s health may help parents become a buffer for that impact - With the right tools, children can thrive despite having experienced trauma
Having ACEs in Your Past Doesn’t Have to Define Your Future
While ACEs are clearly related to health and behaviors later in life, they aren’t a guarantee of anything. The negative health effects of ACEs can be buffered by increasing individual and community- level protective factors that build resilience, for example:
- Building skills in practices such as mindfulness, goal setting, positive coping, and conflict
resolution - Eating well, getting plenty of sleep, and staying active
- Caring relationships with parents, teachers, counselors, or others actively involved in a child’s life
- Safe, stable, and nurturing relationships and environments 7
Data Snapshot: Trends & Disparities
A person with four or more ACEs is:
- 21% as likely to live at or below 250 percent of the Federal Poverty Level (FPL) 4
- 27% as likely to have not graduated college 4
- 39% as likely to be unemployed 4
16.3% of California adults reported having been exposed to four or more Adverse Childhood Experiences (ACEs) before the age of 18. 10
- 27 out of 58 counties (46.6%) in California were above the state average prevalence of adults reporting having been exposed to four or more ACEs 10
- Humboldt, Trinity, Kings, and San Benito counties had the highest reported prevalence of adults reporting having been exposed to four or more ACEs 10
Proportion of Children Who Are Exposed to Adverse Experiences (Parent Reported)
Proportion of Respondents Who Have Been Exposed to Adverse Childhood Experiences Before the Age of 18 (Adult Retrospective)
|
Share Your Story
Want to engage in moving the dial on Healthy Beginnings? Share your impact story!


