Reducing body mass index (BMI) by 5 percent could save California billions
If adult body mass index (BMI) were reduced by 5%, California could save $81.7 billion in obesity-related health care costs by 2030.1
Obesity increases the risk of many health conditions and contributes to some of the leading causes of preventable death, posing a major public health challenge.2 There are many factors that contribute to weight gain and ultimately to obesity. Inactivity, unhealthy diets, and eating behaviors are the most preventable. The rising rates of obesity are related to health conditions such as diabetes, heart disease, high blood pressure, and stroke.2
Indicator Progress
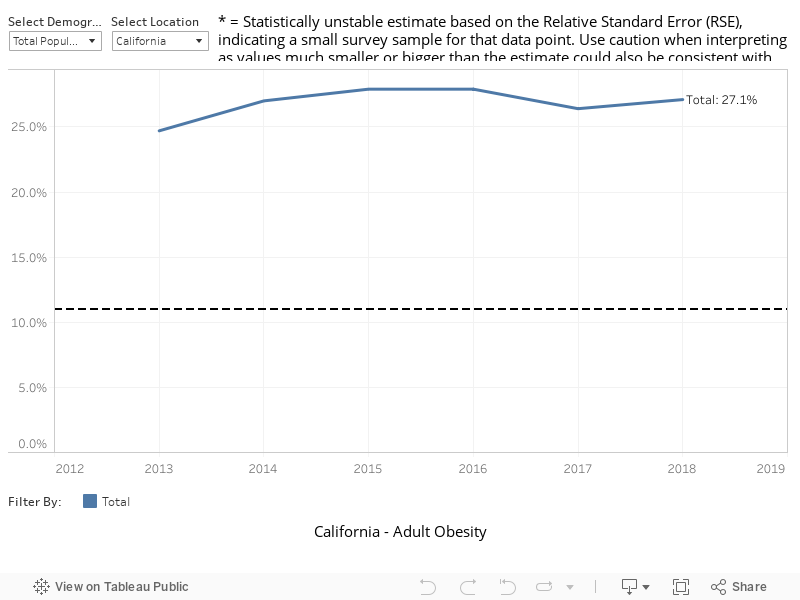
In 2009 (baseline year), 22.7% of adults were obese. The current value in 2018 was 27.1%. The updated 2034 target is to be determined (TBD).
More Data about Obesity – Adult Obesity
Adult Obesity
Note: The data source has changed from the original LGHC 2012 Task Force Report as the original data source is no longer available.
Baseline
22.7%
Target
TBD
Indicator Highlights

Growing Healthy Habits – A Community Garden Model
Yolo County Health and Human Services Agency has established a community garden at the agency’s Bauer building. This community garden provides an opportunity for residents to grow and eat fresh fruits and vegetables and a demonstration space for garden-based education programs. This program aims to build a healthy community by reaching out to families that have limited access to fresh produce and healthy foods. Read more »
California has the highest obesity-related costs in the United States, estimated at $15.2 billion annually.2
By 2012, 21 of California’s 58 counties had adult obesity rates at or above the national Healthy People 2020 goal of 30.5% or more, compared to none of the counties in 2001.2
Nearly half of the added sugars consumed by Americans come from sugar-sweetened beverages. In addition, meals from fast food are often more calorie-dense and less nutritious than meals cooked at home. There is some evidence that indicates limiting consumption of sugar-sweetened beverages and fast food may reduce the risk of weight gain and obesity.2
Only one-quarter of adults achieve the guidelines for physical activity.2 Lack of access to safe places to exercise in neighborhoods and busy work schedules are barriers to physical activity and play a large role in a person’s likelihood for becoming obese.2
Over one-third of adults in California reported that they seldom, never, or only sometimes could find a variety of good quality, affordable fresh fruits and vegetables in their neighborhood.2
Breastfeeding has been shown to have a protective effect against obesity. Children who have been breastfed have less risk of becoming overweight or obese, even as adults.3
Disparities & Trends
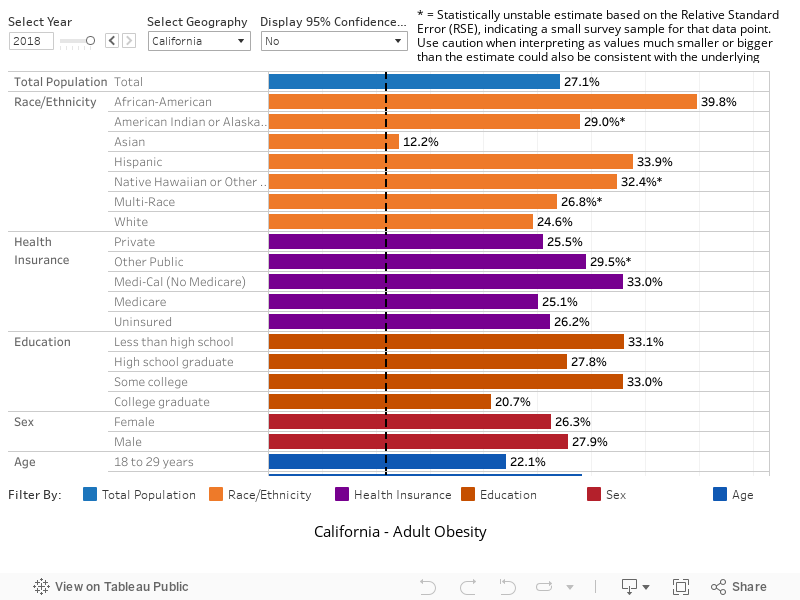
Significant health disparities continue to exist. The rates of obesity are highest among those with low income and lowest among higher income Californians.2
Individuals who are obese have medical costs that are $1,429 per year higher, or roughly 42% greater, than the costs of those with normal body weight.2
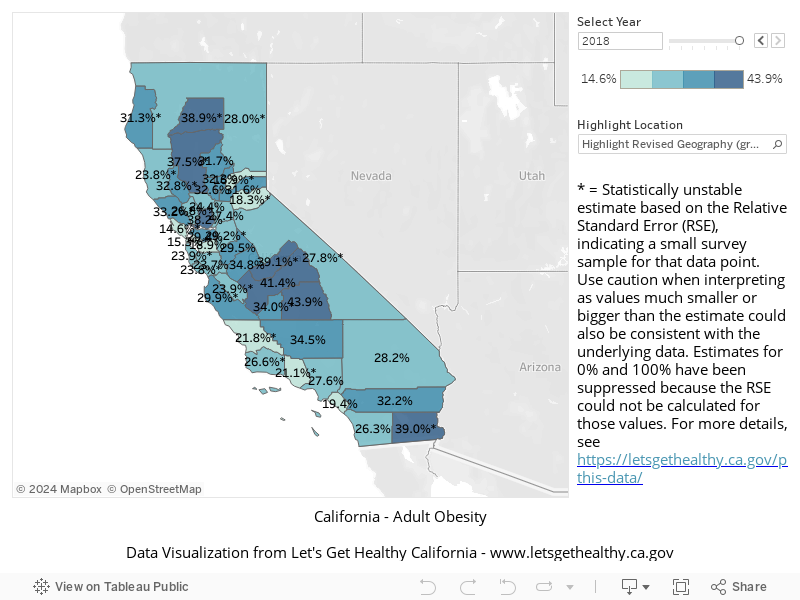
One in three counties in California has an obesity rate higher than the national Healthy People 2020 goal.2
Obesity varies significantly by county in California. Only 11.3% of adults living in San Francisco County are obese compared with 41.7% of Imperial County adults.2
Annually there are nearly a half million hospital admissions due to obesity-related conditions in the State, accounting for $33.8 billion in hospital charges.2
Obesity has also been linked with reduced worker productivity, chronic absence from work, and medical spending that totals $73.1 billion per year for full time employees in the United States.2
Proportion of Adults Who are Obese, Over Time
Proportion of Adults Who are Obese, by Demographic Category
Proportion of Adults Who are Obese, by County
|
Stories & Solutions
Increasing Breastfeeding Duration
If 90% of US families could comply with current medical guidelines to breastfeed exclusively for 6 months, the US could avoid about $18.5 billion per year in increased health care costs (2014 dollars). 1 The multiple health benefits of exclusive breastfeeding for both the infant and mother are well [...]
Growing Healthy Habits – A Community Garden Model
Yolo County Health and Human Services Agency has established a community garden at the agency’s Bauer building.

Market Makeovers Increase Access to Fresh Produce
Connecting a corner store, a farmers market, and a refrigerator to increase access to fresh produce for the L.A.’s Historic Filipinotown community. Historic Filipinotown is a community in the City of Los Angeles where the availability of and access to fresh produce is limited; 17 out of 25 small stores [...]

Rethink Your Drink
This public health initiative aims to educate low-income Californians about healthy drink options, help identify drinks with added sugar, and make the link between consumption of sugar-sweetened drinks and health risks.

Transportation and Community Plans that Promote Walking and Healthy Eating
Collaboration between residents, city council and city planners improves walkability between a corner store and elementary school.

Safe Routes to Healthy Places – San Diego County
The Healthier Me Initiative and creating policy, systems, and environmental change,
Share Your Story
Want to engage in moving the dial on the Living Well goal? Share your impact story!


