Breastfeeding helps build the foundation for a healthy life, providing benefits for infants and breastfeeding parents
Although most newborns breastfeed (or receive breast milk) during their first day of life, few are exclusively breastfeeding at six months old. Breast milk contains nutrients, antibodies, and other essential ingredients that protect infants from infections and promote brain development and digestive health. Over the life course, those who were breastfed have reduced risks of ear infections, asthma, childhood obesity, and type 2 diabetes. Breastfeeding parents have reduced recovery time after delivery and, over the life course, lower risks of ovarian and breast cancer, high blood pressure, and type 2 diabetes.
The American Academy of Pediatrics and the World Health Organization recommend exclusive breastfeeding for the first six months, with continued breastfeeding for at least two years or beyond, balanced with the introduction of foods. Exclusive breastfeeding consists of only breast milk, without any additional food or liquids, not even water.1,2
This indicator tracks exclusive breastfeeding at 3 months postpartum.
Breastfeeding
In 2019-21 (baseline years), exclusive breastfeeding at 3 months postpartum was 32%. The most recent data available indicate 32% (2019-21). We hope to reach a target of 41.6% or higher by 2034.
Baseline
32.0%
Target
41.6%
Data Snapshot
Parents with lower household income are less likely to exclusively breastfeed at three months postpartum than those with higher household income.
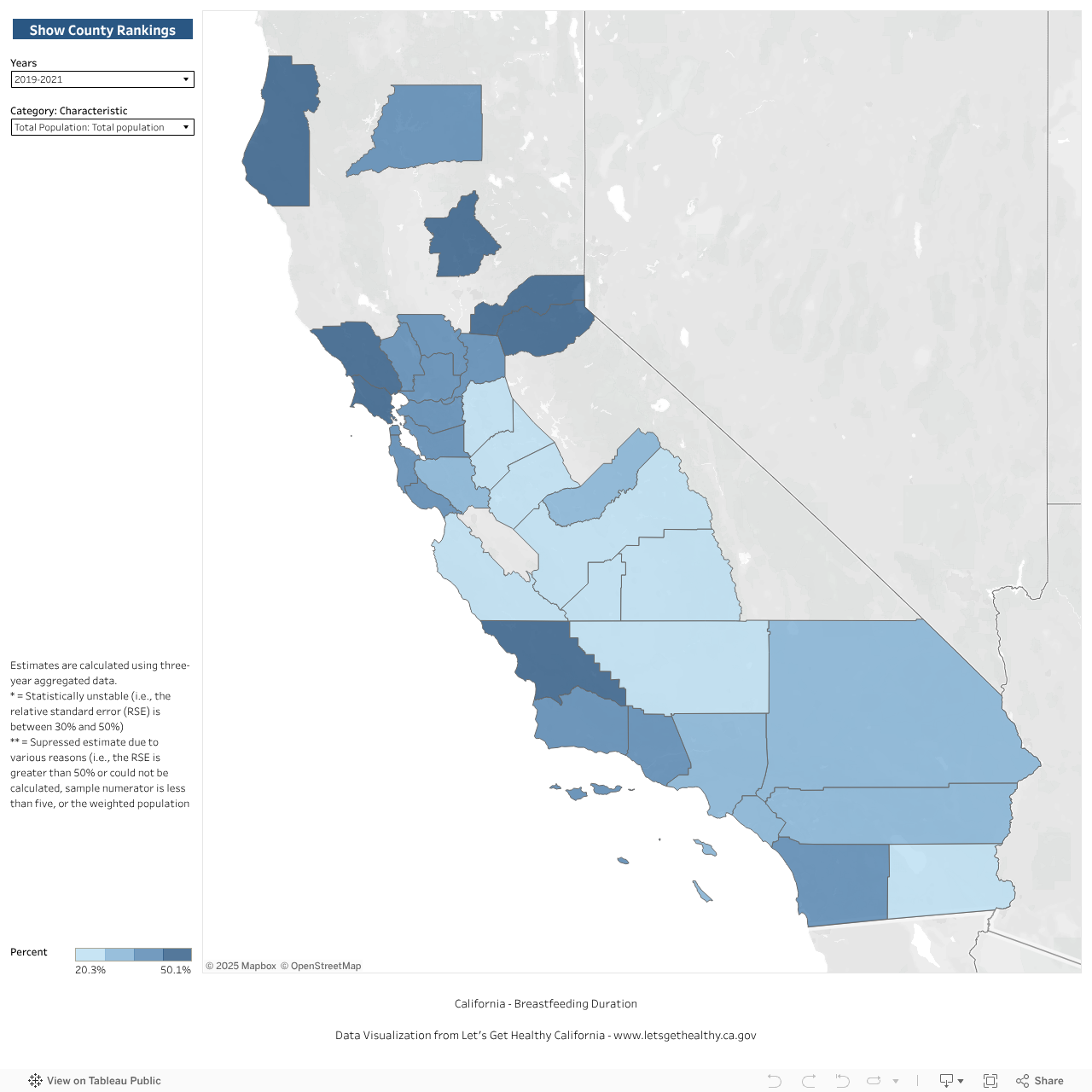
Exclusive breastfeeding varies significantly by county. Among the counties with reliable data, several Southern and Central Valley counties report much lower exclusive breastfeeding than the rest of California.
White birthing individuals are more likely to exclusively breastfeed at three months postpartum compared to other race/ethnic groups.
Exclusive Breastfeeding at 3 Months Postpartum, Over Time

Exclusive Breastfeeding at 3 Months Postpartum, by Demographic Category

Exclusive Breastfeeding at 3 Months Postpartum, by County
|
Share Your Story
Want to engage in moving the dial on Healthy Beginnings? Share your impact story!
More From Let’s Get Healthy California


