Hospital readmissions cost the nation billions each year.1
Hospital readmissions refer to a hospital stay that occurs shortly after a patient has been discharged from the hospital. Hospital readmissions that occur within a short amount of time following a hospital discharge are a measure of clinical quality.1 High rates may indicate low quality care either during the hospital stay or after discharge, and are associated with high costs.2
This indicator tracks unplanned hospital readmissions within the first 30 days after hospital discharge.
Hospital Readmissions
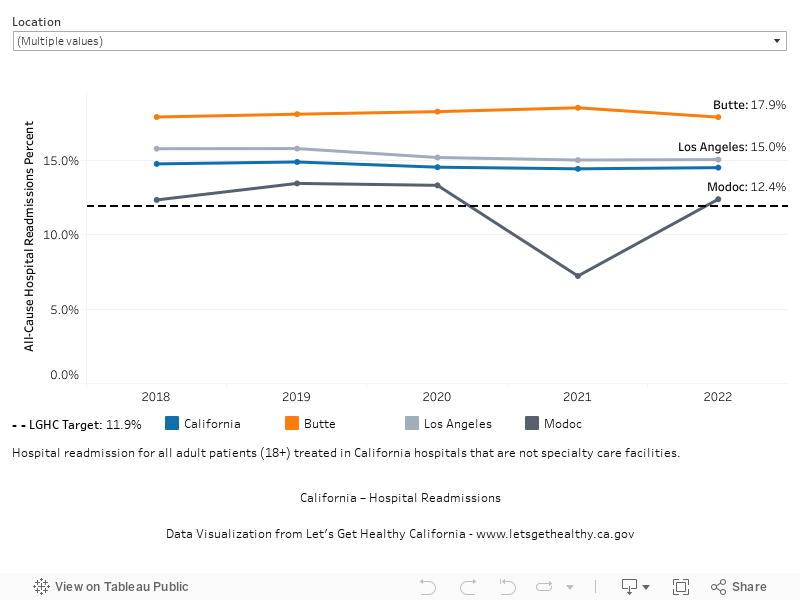
In 2022 (baseline year), 14.5% of hospital discharges resulted in unplanned readmissions within 30 days. The most recent data available show 14.5% (2022). We hope to reach a target of 11.9% or lower by 2034.
More Data about Hospital Readmissions
Hospital Readmissions
Note: The target has changed from the original LGHC 2012 Task Force Report; see footnote on indicator page.
Baseline
14.5%
Target
11.9%
Indicator Highlights
Hospital readmissions cost 12.4% more on average than the cost of the previous hospital stay.3
In 2020, six condition groups accounted for 1 in 3 hospital readmissions: circulatory system diseases; infectious and parasitic diseases; digestive system diseases; injury, poisonings, and other external causes; respiratory system diseases; mental, behavioral, and neurodevelopmental disorders.3
Medication management
Medication review and reconciliation by pharmacists can reduce adverse drug events that contribute to hospital reamission.4,5
Financial incentives
Financial penalties to hospitals in the Affordable Care Act (ACA) for high hospital readmission rates have been linked to declines in hospital readmissions with no corresponding increase in deaths within 30 days of discharge.6
Patient-centered care
Dedicated transition providers, information sharing, and improved care coordination between hospital and community providers are associated with fewer hospital readmission.4,7
Data Snapshot
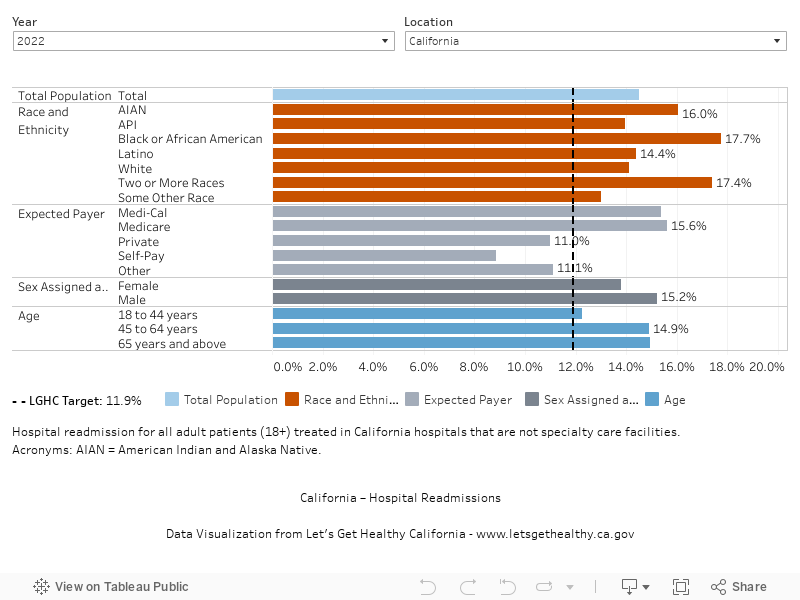
Hospital readmission rates are higher for patients with Medi-Cal and Medicare than for other expected payers. 3
In 2022, readmission rates by race and ethnicity were higher for Black, American Indian and Alaska Native, and multiracial Californians than for White Californians.
Rate of Unplanned Hospital Readmissions Within 30 Days of Discharge, Over Time
Rate of Unplanned Hospital Readmissions Within 30 Days of Discharge, by Demographic Category
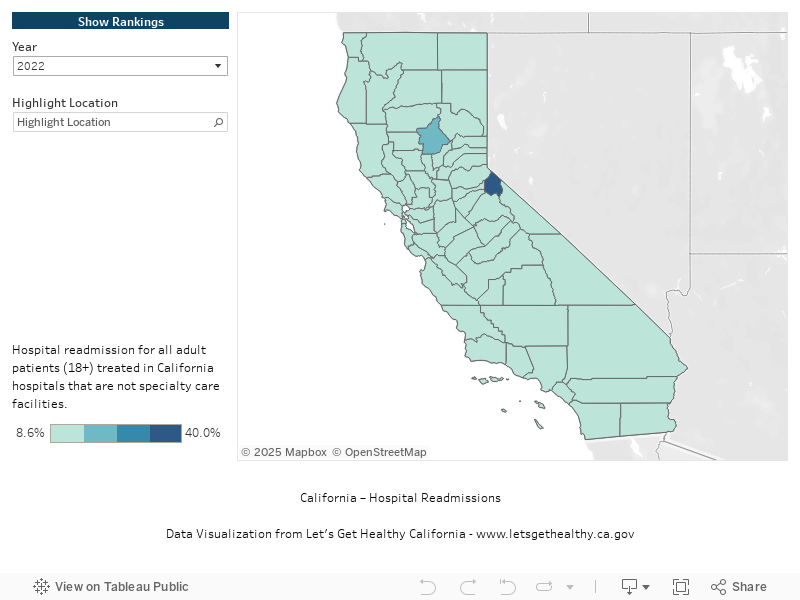
Rate of Unplanned Hospital Readmissions Within 30 Days of Discharge, by County
|
Stories & Solutions

The California HealthCare Foundation highlights nine examples of patient-centered programs to reduce readmissions
CHCF highlighted two exemplary California Programs including: 1) Sharp Rees-Stealy Medical Group reduced hospital readmissions and generates a positive return on investment by using nurse case managers to improve the transition of care process for high-risk patients; and 2) Blue Shield of California developed a patient-centered management program that used [...]

Centers for Medicare & Medicaid Services (CMS) has implemented incentives to reduce hospital readmissions
Under the Affordable Care Act, CMS has implemented the Hospital Readmission Reduction Program (HRRP) which aims to reduce preventable hospital admissions by penalizing hospitals with relatively higher rates of Medicare insured readmissions. Since implementation of the HRRP, reducing hospital readmissions has gained traction among providers and policymakers. Evaluating the HRRP [...]
Share Your Story
Want to engage in moving the dial on the Redesigning the Health System goal? Share your impact story!


