Millions of Californians haven't communicated their choices for end-of-life care.1
End of life is one of the most difficult stages of life and is in need of attention to improve the care and experience of individuals who are dying. Many patients at the end of life could benefit from palliative care.
Palliative care is specialized, team-based care that focuses on relieving symptoms and improving quality of life for both the patient with a serious illness, and the patient’s family.1 It can be provided at any stage of a serious illness, and can be provided together with curative treatment. Further, providers of these services work with other health care team members to make sure that the care that is delivered is aligned with patient goals, values, and preferences.
Tracking the percentage of California hospitals that provide in-patient palliative care helps to make sure that hospitalized patients with serious illness receive care that meets their physical, emotional, and spiritual needs.
Indicator Progress
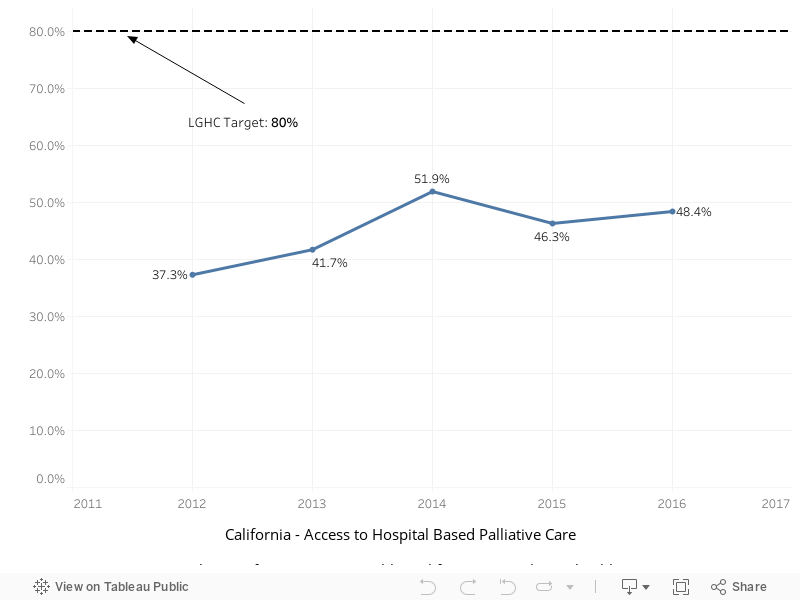
In 2012 (baseline year), 37.3% of California hospitals provided in-patient palliative care. The current value in 2016 was 48.4%. The updated 2034 target is to be determined (TBD).
More Data about Access to Hospital Based Palliative Care
Access to Hospital Based Palliative Care
Note: The data source has changed from the original LGHC 2012 Task Force Report as the original data source is no longer available.
Baseline
37.3%
Target
TBD
Indicator Highlights

Death Over Dinner
Parties where participants have dinner together and created a safe place to have the conversation about the end of life. Learn More »
80% want to talk
In a 2011 survey by the California HealthCare Foundation (CHCF), nearly 80% of Californians said they would “probably or definitely want to talk with their doctor if they were seriously ill”2
7% discussed with doctor
Although most patients said they want to discuss these issues, only 7% said their doctor ever raised the topic.2
23% written down
Only 23% of Californians surveyed said they had written down their end of life wishes.2
In the past ten years, a growing body of evidence that palliative care improves patient outcomes has led to a steady increase in the number of hospital-based programs nationally. Still, not all hospitals offer such services.
Key factors affecting access to in-patient palliative care programs include availability of certified/designated palliative care providers and focus and prioritization of palliative care.4
Disparities & Trends
In California, the availability of in-patient palliative care has been increasing in recent years. The Let’s Get Healthy California indicator shows that 52% of hospitals currently offer palliative care programs, moving toward the 80% target for 2022.
Note that alternative measures for this topic have found that 74% of California’s hospitals with 50 or more beds had palliative care programs in 2012 or 2013.
Some hospitals, particularly smaller hospitals or those in rural parts of the State, do not yet have palliative care programs.5
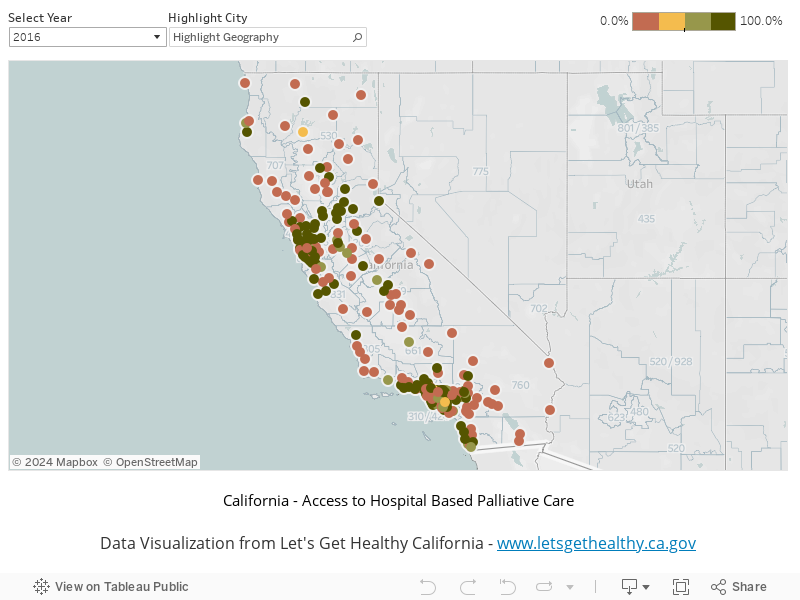
Percent of California Hospitals Providing In-patient Palliative Care by City
Percent of California Hospitals Providing In-patient Palliative Care, by City
|
Stories & Solutions

Innovation Conference: End of Life Breakout Session
Moderated panel discussion among Innovation Challenge finalists on interventions to address End of Life.
Medical-Legal Partnership for Seniors
The Medical-Legal Partnership for Seniors provides legal assistance to lower income adults assisting them with health and financial advice, as well as advance care planning.
Aging With Dignity at Home
Aging with Dignity at Home, AltaMed’s Program of All-Inclusive Care for the Elderly (PACE) allows seniors to receive coordinated medical, social, dental, nutritional and rehabilitative services, including Adult Day Health Care (ADHC) close to their homes and within the community.
UCLA Health/Coalition for Compassionate Care of California Advance Care Planning Initiative (ACPI)
The Coalition for Compassionate Care of California (CCCC) is partnering with the UCLA Health System to develop and test an innovative comprehensive advance care planning model that routinely receives patient preferences through a standardized process that ensures that these preferences are recorded and that they can be retrieved and honored at critical times.
Death Over Dinner
Parties where participants have dinner together and created a safe place to have the conversation about the end of life.

Being Mortal
Frontline explores the intersection of life, death, medicine, and what matters in the end.


Palliative Pooches: When Dogs Make the Rounds
Learn about the service that therapy dogs provide by supporting and comforting patients and doctors in palliative care settings.
Dying in California: A Status Report on End-of-Life Care
Dying in California serves as a snapshot of the state's progress in end-of-life care, as measured against the recommendations made in the Institute of Medicine's influential 2014 report Dying in America: Improving Quality and Honoring Individual Preferences Near the End of Life.
Share Your Story
Want to engage in moving the dial on the End of Life goal? Share your impact story!


