National health spending growth is expected to accelerate 5.7 percent for 20171
The overall cost of health care includes more than just out-of-pocket costs and insurance premiums. Tracking California’s compound annual growth rate (CAGR) of health care spending is one way to monitor the overall cost of care. This indicator is valuable as it includes past trends in rate of spending on health care, and also helps predict what the rate of spending is going to look like in the near future.
The Let’s Get Healthy California goal is to bring California’s growth rate of health care expenditures in line with the rate of growth in Gross State Product (GSP) by 2022.
Indicator Progress
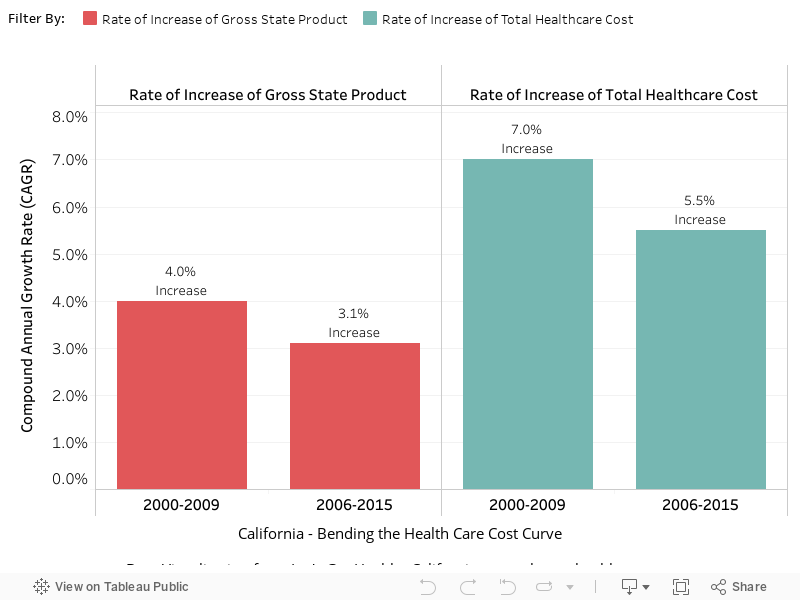
In 2012 (baseline year), the rate of increase of total healthcare cost was 7.0%. The current value in 2015 was 5.5%. The updated 2034 target is to be determined (TBD).
More Data about Health Care Spending Growth Rate by Total Health Expenditures
Baseline
7.0%
Target
TBD
Indicator Highlights
Health care in the coming years is expected to become increasingly more expensive for families, employers, and federal and state governments.4
A primary concern is the high growth rate in average
health care expenditures.
The Centers for Medicare and Medicaid Services (CMS) projects national health spending to grow 1.3 percentage points faster than Gross Domestic Product (GDP) per year from 2015-2025; as a result, the health share of GDP is expected to rise from 17.5 percent in 2014 to 20.1 percent by 2025.1
Data Snapshot: Trends & Disparities
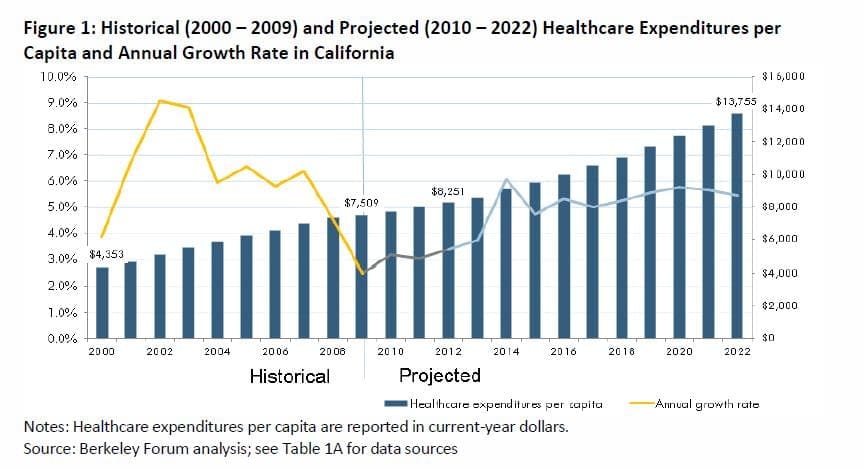
Between 2000 and 2009, per capita health care expenditures in the state grew at an average annual rate of 6.3%, from $4,353 to $7,509. The annual per capita growth rate began decreasing near the end of the decade, falling to 2.5% in 2009, largely due to the 2008-2009 recession.3
Compound Annual Growth Rate by Gross State Product and Total Healthcare Cost
The growth rate of health care expenditures is calculated over an interval of time. For this data visualization (below), the CAGR is displayed as a comparison of the most recent 10-year interval (2006-2015) with the 10-year interval calculated in the 2012 Task Force report (2000-2009). Viewing a broader interval increases stability of the CAGR output value.
|
Share Your Story
Want to engage in moving the dial on the Lowering the Cost of Care goal? Share your impact story!


